This 69 year-old male patient presented to a chiropractor with acute onset low back pain. He has a history of prostate cancer dating back to 2015. The patient had received 3 adjustments before x-rays were available, and he reports that his pain is lessening with care.
Figure 1: Note marked universal osteoporosis, with collapse of the L1 body along its entire sagittal dimension; it is not wedge-shaped
Figure 2
Figure 3
Figure 1
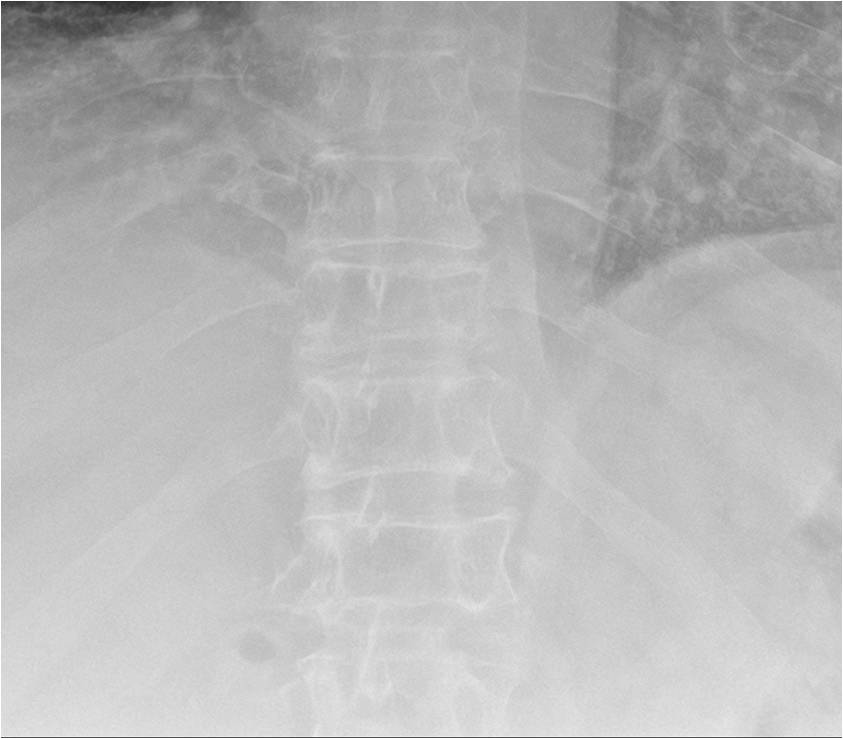
figure 2. AP thoracic
On x-ray: note the general osteoporotic spine. Of key importance is the decrease in vertical height of both the T11 and L1 vertebral bodies, as seen on the AP projection. No lateral thoracic was submitted, but the lateral lumbar clearly shows complete collapse of L1. The important feature is decreased posterior body height. This helps differentiate this fracture from a simple osteoporotic compression fracture, also common in this same age group. Due to a greater amount of trabeculation in the posterior aspect of a vertebral body, an osteoporotic vertebral body classically presents as trapezoidal on a lateral film, demonstrating anterior wedging. A pathological collapse, as in this patient, will additionally demonstrate decreased posterior body height, not a good sign. I recommended a bone scan as soon as possible to further evaluate the entire skeletal status. As an interesting aside, you may remember that metastasis from a prostate primary is classically blastic, but tumors don’t read the textbooks!
Figure 3. Close-up of AP thoracic; showing compression of both the T11 and L1 vertebral bodies
Marshall Deltoff DC, DACBR, FCCR(Can) FEAC, Professor of radiology, Barcelona College of Chiropractic; marshdel@yahoo.ca